
Congenital Heart disease as a name and extent of disease load in our country was unheard of in my life till I started working with children affected by this life threatening disease. Although the science background that I came from had made me aware of the term congenital, which means presence of something from birth. Diseases can be acquired during life time from the environment and other sources but congenital are those defects or diseases which precipitate during fetal growth in the womb. There are various developmental abnormalities that occur during fetal growth. These abnormalities can be of various types. It can be abnormality in the walls of the four chambers of heart, Abnormality in the valves between the chambers and it can also be abnormality in the blood vessels of the heart. Seeing few days old babies make it and survive while few unfortunate ones who do not, has changed my outlook towards life !

The statistics of 1 child born in every 100 live births with any of these abnormalities is alarming. Although this data is common all over the world but with the population and resources we have as a developing country, this is HUGE! We lack the number of hospitals with dedicated pediatric cardiology departments, lack of pediatric cardiac specialists for diagnosis and the pediatric cardiac surgeons for treatment. Out of 200000 children born every year with this defect, only 15000 get to access treatment, which leaves the rest to die or wait.
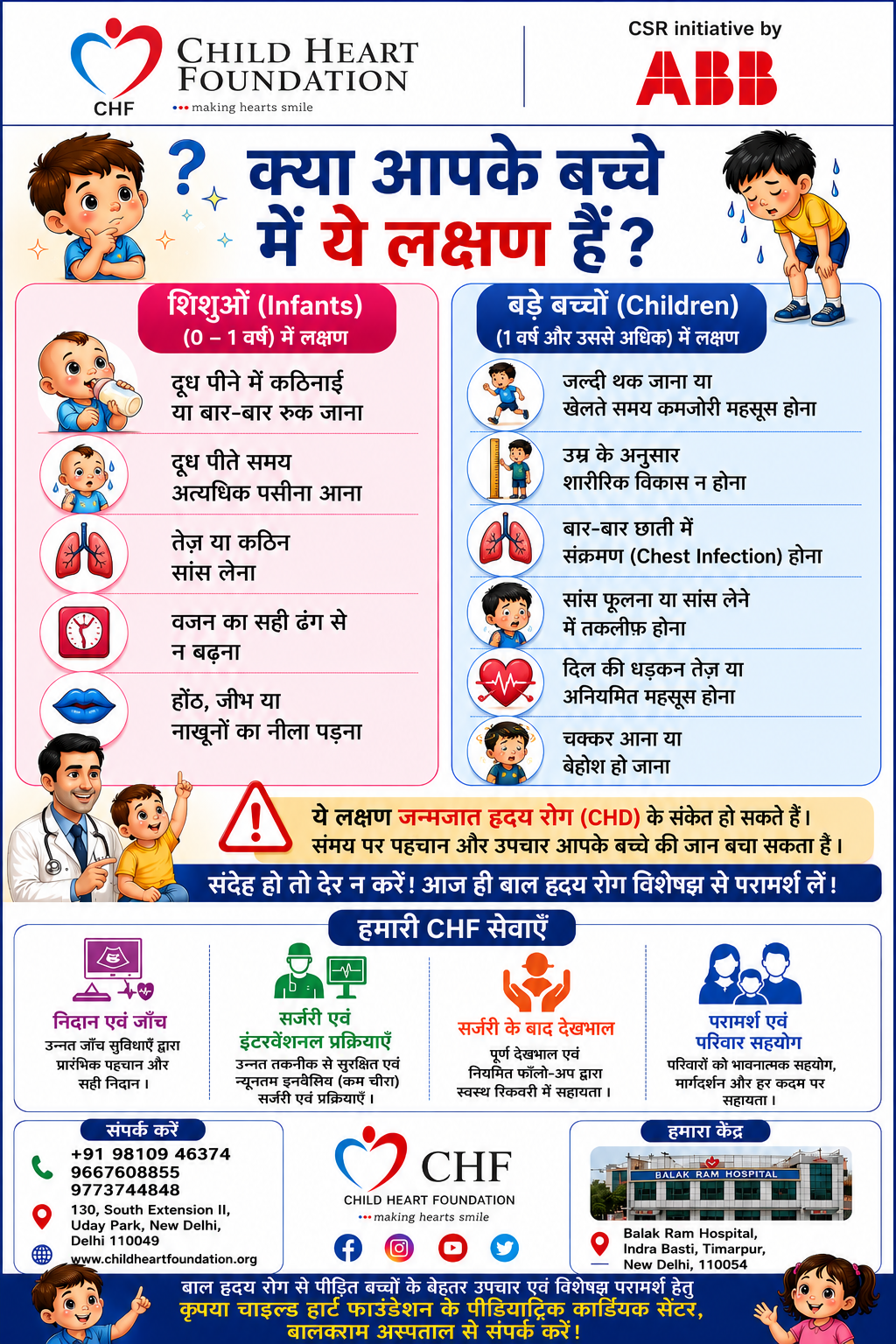
There is delay in diagnosis and reporting because of lack of awareness due to high illiteracy in general masses in rural areas. People are ignorant of the symptoms for early reporting. Thus the symptoms get ignored and over a period of time when the problem gets worse, it becomes unmanageable.
There is delay in diagnosis and reporting because of lack of awareness due to high illiteracy in general masses in rural areas. People are ignorant of the symptoms for early reporting. Thus the symptoms get ignored and over a period of time when the problem gets worse, it becomes unmanageable.
Access to Governmental set ups is open to all but because of high numbers of patients, chance of getting an appointment or date for treatment becomes a challange. Parents are issued dates of 2 to 3 years ahead, while in reality, the treating doctors know that the child in question would not be able to survive and make it till his future assigned date.
All this leaves the parents with no hope but to knock on the private commercial healthcare setups. The highly expensive treatment for this disease, leaves parents with no choice but to suffer and live with the trauma and guilt of losing their child in front of their eyes due to lack of funds.
Pivate Insurance agencies are of no help as congenital heart diseases are considered as pre existing defects so don't come under the insurance cover.
Pivate Insurance agencies are of no help as congenital heart diseases are considered as pre existing defects so don't come under the insurance cover.

Government has come up with various health schemes, prominent among them being RBSK scheme. It covers CHD as well. According to this scheme, no child should die due to CHD. It sounds wonderful, but, we all know the fact that for no child to die due to CHD, it is very important to carry out early detection and screening at each and every district of our country. For this to happen, RBSK has suggested making DEIC ( District Early Intervention Centers ) which would carry out early screening for CHD. But, the fact remains, to carry out early detection/screening, we need trained medical professionals for early detection.
The number of pediatric cardiologist as of now in our country is just 250-270. How can we imagine these numbers to cater to population in crores?
The number of pediatric cardiologist as of now in our country is just 250-270. How can we imagine these numbers to cater to population in crores?
We need to train other medical fraternity to address this problem. We need to train technicians to operate echo machines to carry out early diagnosis. We need to create some programs to engage with basic community workers for talking to people about CHD and make them aware when to seek help based on symptoms seen in their child.
The only solution to address this is
1. Create awareness and sensitization about the disease and disease load amongst people
2. Train more health professionals for early screening and diagnosis
3. Built more Government and Charitable hospitals with dedicated Pediatric Cardiology Departments
1. Create awareness and sensitization about the disease and disease load amongst people
2. Train more health professionals for early screening and diagnosis
3. Built more Government and Charitable hospitals with dedicated Pediatric Cardiology Departments